In January 2026, the FDA cleared the first cell reprogramming therapeutic drug for human testing with the implicit goal of reversing aging. Specifically, the agency cleared ER-100, a therapy designed to treat optic nerve conditions, including glaucoma and non-arteritic anterior ischemic optic neuropathy, to be tested on human patients. Optic nerve conditions, which are thought to be caused by aging, cause damage to the retinal ganglion cells (RGCs) of the eye. The trial, which will last five years, is considered an important step forward for epigenetic therapies to reverse cell damage. More significantly, it is also a landmark trial for therapies designed to slow, stop, or reverse aging.
Anti-aging medicine is a field that has emerged in academia, the pharmaceutical industry, and the commercial wellness space over the last decade as part of a wider cultural shift in medicine from reactive to preventive care. Putting the approval and eventual results of the ER-100 trial in context requires an understanding of the anti-aging field at large, including what trials can and cannot prove, the regulatory backdrop for reaching customers, and the landscape of scientific approaches to other therapies that may fall in this bucket.
While both academic and commercial endeavors to slow, stop, and reverse aging are consistently attracting increasing funding, the field has yet to recover from public failures in previous hype cycles or gain widespread traction with consumer usage. The success of newer research experiments and clinical trials may meaningfully accelerate continued funding in this space, even as both technical and regulatory guidelines are still being drawn.
Geroscience vs. Longevity
It is worth noting up front that geroscience, the interdisciplinary study of age-related chronic diseases and the biological pathways that trigger them, as practiced in academic labs and pharmaceutical pipelines, is a fundamentally different enterprise from the longevity content economy that is concurrently growing. To better parse the distinctions between these spaces, it is useful to separately define aging, longevity, and rejuvenation.
Aging refers to the underlying biological processes that collectively raise the risk of chronic diseases in humans over time. These include genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, deregulated nutrient-sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, and altered intercellular communication (as characterized in Hallmarks of Aging, the leading catalog of aging-related biological markers published by Lopez-Otin et. al. in the journal Cell).
Longevity is the downstream outcome of aging, measured clinically by the number of years lived. A related distinction exists between the concepts of lifespan and healthspan, both of which may be extended by the interventions that aging researchers are developing:
Lifespan is the total number of years of life duration from birth to death. While lifespan is easy to define, it is difficult to study in real-time trials because participants may live for years or decades beyond the beginning of a study and may encounter confounding health factors throughout that period.
Healthspan is the total years lived free of significant disease or disability. Healthspan is what most patients and clinicians actually care about, and it is what geroscience-oriented trials are designed around.
Academic and pharmaceutical industry geroscience researchers are largely less focused on longevity (as a noisy output of thousands of cross-cutting biological processes evolving concurrently) and more on the tracking of specific biomarkers associated with aging. Wellness influencers focused on longevity interventions, however, have gained significant followings in recent years, often making grand and unsubstantiated claims about increasing human lifespan via practices that have not been scientifically tested.
Rejuvenation is the reversal of biological aging (as measured by age-related biomarkers), distinct from just slowing its accrual. As of June 2026, rejuvenation has been demonstrated in mice through partial cellular reprogramming and parabiosis experiments, but has not been verifiably tested in humans.
While academic geroscientists study the mechanisms that control aging and rejuvenation, influencer protocols often conflate all three, treating changes in biomarkers as equivalent to reversal of aging or extended lifespan when these correlations between interventions are still being validated.
Longevity Hype Cycles
ER-100 is not the first attempt at a major breakthrough within geroscience. Several prior cycles revolving around different technologies each produced clinical disappointments, but provide important context for thinking through the eventual results of the ER-100 trial and others that may take place in the future.
Telomerase (1998-2010s)
Geron Corporation, founded in 1990, and Bill Andrews at Sierra Sciences both pursued telomerase activation as a strategy to extend cellular lifespan, building on the Hayflick Limit discovery that telomere shortening drives replicative senescence. After Geron-funded researchers showed that introducing the hTERT gene into normal human cells extended their replicative lifespan indefinitely without making them cancerous, the company pursued telomerase activation as an anti-aging strategy.
This work largely stayed at the level of cell biology, preclinical research, and licensing, and the company never ran human clinical trials of a telomerase activator for aging indications. The closest thing to a clinical product in this lineage was TA-65, a small-molecule telomerase activator derived from astragalus that Geron licensed out to TA Sciences, which sells it as a nutraceutical rather than developing it as an FDA-regulated drug as of June 2026. Bill Andrews pursued a parallel screening effort for telomerase activators but likewise never brought one to clinical trials for aging.
The fundamental problem with this approach was that telomerase is one common indicator of cancer: roughly 90% of human malignancies upregulate telomerase to achieve replicative immortality, meaning any systemic activator risks promoting tumorigenesis. Geron pivoted to oncology in the mid-2000s, abandoning anti-aging development to pursue the opposite mechanism, inhibiting telomerase to selectively kill cancer cells dependent on it. The company eventually developed imetelstat, approved in 2024 as RYTELO for transfusion-dependent anemia in lower-risk myelodysplastic syndromes.
Resveratrol / Sirtuins (2003-2013)
The sirtuin-activator program was the most heavily capitalized therapeutic effort in the modern aging field. The scientific basis for the treatment originated in a 2003 finding from David Sinclair's lab that resveratrol, a polyphenol, increased the catalytic activity of the NAD⁺-dependent deacetylase SIRT1 and extended replicative lifespan in Saccharomyces cerevisiae (Nature 2003), positioning it as a small-molecule mimetic of caloric restriction.
Sirtris Pharmaceuticals was co-founded by Sinclair to develop synthetic sirtuin-activating compounds (STACs) such as SRT1720 (which are structurally unrelated to resveratrol), which reportedly activated SIRT1 with far greater potency than polyphenols. GSK acquired the company for $720 million in 2008, with the sale including a pipeline of structurally distinct next-generation STACs and then-leading clinical asset SRT501, a proprietary micronized formulation of resveratrol intended to improve its low oral bioavailability.
The trajectory of sirtuins illustrates the risk of building a platform on a mechanism observed purely in-vitro; the claim was subsequently attributed to an assay artifact. Groups at Amgen (2009) and Pfizer (2010) reported that the apparent activation depended on the use of a non-native peptide substrate conjugated to a fluorophore; the compounds enhanced deacetylation only in the presence of the fluorescent tag and showed no activation against native untagged substrates, indicating that the measured effect reflected substrate-fluorophore interaction rather than allosteric activation of the enzyme.
On the clinical side, GSK discontinued SRT501 after reports of nephrotoxicity, including renal failure, in a trial in multiple myeloma patients, where the formulation was also judged to lack sufficient efficacy. GSK closed Sirtris in 2013 and folded its remaining activities into internal R&D. The story of an enzyme-activation mechanism that did not replicate on physiological substrates, followed by a formulation discontinued on safety and efficacy grounds, is frequently cited in discussions of why subsequent geroscience trials (TAME, ASPREE, the Loyal programs) have been designed around clinical endpoints rather than biochemical or enzyme-activation surrogates.
Rapamycin (2009-2025)
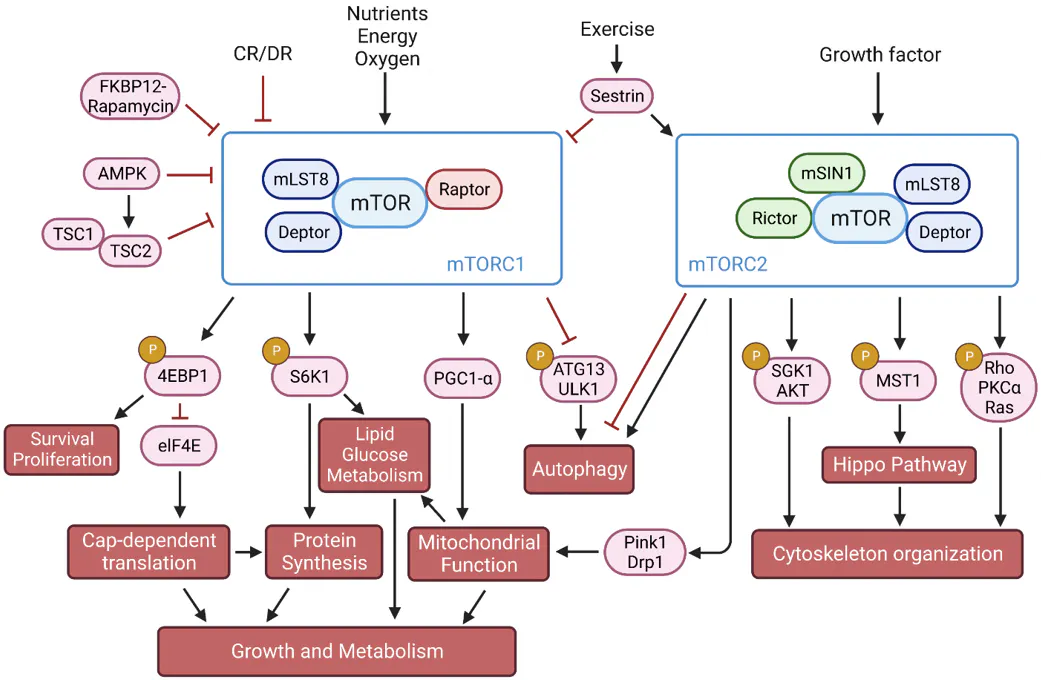
The most extensively replicated lifespan-extending intervention in any mammal is rapamycin, a macrolide originally isolated from Streptomyces hygroscopicus in Easter Island ("Rapa Nui") soil samples and developed as the immunosuppressant sirolimus. Rapamycin inhibits mTORC1, a nutrient-sensing kinase complex that genetic studies in yeast, C. elegans, and Drosophila had previously implicated in control of organism lifespan.
The NIA Interventions Testing Program, a three-site randomized protocol run in parallel at the Jackson Laboratory, UT Health San Antonio, and the University of Michigan, first reported in a 2009 study that encapsulated rapamycin fed to genetically heterogeneous (UM-HET3) mice from 600 days of age (roughly the murine equivalent of age 60 in humans) extended median and maximum lifespan in both sexes. The result has since been replicated across multiple doses, multiple starting ages, and intermittent dosing schedules, with effect sizes ranging from 9–26% extension of median lifespan depending on regimen. No other intervention has accumulated comparable depth of independent mammalian replication.
Human translation trials have proceeded along two distinct tracks, both targeting age-related immune decline as a tractable proxy for "aging" rather than aging-as-construct. The first track used everolimus (RAD001), a structural analog of rapamycin. In a 2014 study, a Novartis-sponsored Phase 2a trial in 218 adults aged 65+ showed that low-dose RAD001 improved influenza vaccine antibody response by approximately 20% and reduced te proportion of PD-1-expressing exhausted T cells, providing the first human evidence that mTOR inhibition could partially reverse immunosenescence. A follow-on Phase 2b study using a combination of RAD001 with the catalytic inhibitor BEZ235 reported reduced respiratory tract infections in 264 older adults, motivating the spinout of resTORbio to develop a selective mTORC1 inhibitor (RTB101) at doses intended to preserve the immune benefit while minimizing the immunosuppression that accompanies higher rapamycin exposure. The pivotal Phase 3 trial, PROTECTOR-1, tested RTB101 against clinically symptomatic respiratory illness in adults 65+ and missed its primary endpoint (odds ratio 1.07, p=0.65); resTORbio merged with Adicet Bio in 2020 and discontinued the program.
The second track is the off-label, low-dose rapamycin use that has spread through the longevity community, formalized in the PEARL trial. The PEARL trial was a 48-week, decentralized, placebo-controlled study testing weekly oral rapamycin against placebo with visceral adipose tissue (VAT) change on DXA as the primary endpoint. PEARL missed its primary endpoint but reported sex-specific secondary findings (increased lean tissue mass and reduced pain scores in women on the highest dose) that have been characterized by the investigators as hypothesis-generating rather than confirmatory.
The commercial trajectory for rapamycin has therefore reverted to the disease-specific indication pattern: Aeovian Pharmaceuticals raised a $55 million Series B in December 2025 to advance AV078, a next-generation selective mTORC1 inhibitor, into Phase 2 for tuberous sclerosis complex–associated epilepsy. Like resTORbio before it, Aeovian's path to approval runs through a specific genetic disease in which mTORC1 hyperactivation is causally implicated, not through aging itself, demonstrative of the recurring pattern in which the most mechanistically promising geroscience targets ultimately advance through narrow disease indications because the regulatory and endpoint infrastructure for aging-as-indication does not yet exist.
Senolytics (2017-2020)
The senolytic hypothesis in aging therapeutics is the idea that selectively killing senescent cells (post-mitotic, secretion-active cells that accumulate with age and drive chronic inflammation via the senescence-associated secretory phenotype, or SASP) would ameliorate multiple age-related diseases. This idea emerged from a series of foundational mouse studies in the early 2010s, most notably studies in 2011 and 2016, from Jan van Deursen's group at the Mayo Clinic, which used genetically engineered mice to clear p16^Ink4a-positive senescent cells and showed extended healthspan and delayed onset of multiple age-related pathologies. The commercial bet on this hypothesis was anchored by UNITY Biotechnology, co-founded in 2011 by van Deursen and other researchers in the field, with backing from investors including Jeff Bezos and Peter Thiel. The company listed publicly in May 2018 at a $700 million market capitalization on a pipeline of small-molecule senolytics targeting BCL-2 family anti-apoptotic proteins that senescent cells depend on for survival.
Both of UNITY's highest-profile clinical programs produced placebo-indistinguishable readouts on their primary endpoints. Both UBX0101 and UBX1325 are senolytics, drugs that selectively kill senescent cells by inhibiting the pro-survival proteins those cells depend on to evade apoptosis. UBX0101, an intra-articular MDM2 inhibitor for painful knee osteoarthritis (chosen as the lead indication because OA is mechanistically tied to local senescent-cell accumulation in cartilage and synovium), failed to separate from placebo on WOMAC pain scores in its Phase 2 readout in August 2020, and the program was discontinued.
The company pivoted to UBX1325 (foselutoclax), a BCL-xL inhibitor delivered intravitreally for diabetic macular edema, which in the ASPIRE Phase 2b trial in March 2025 missed its primary non-inferiority endpoint versus aflibercept (the standard-of-care anti-VEGF therapy). Both compounds targeted disease contexts in which senescent-cell accumulation had been mechanistically implicated, and both failed to separate from comparator on their primary clinical endpoints — leaving open whether senescent cells were not the dominant driver of disease, the compounds did not achieve sufficient clearance at tolerated doses, or the molecules acted more as senomorphics (SASP modulators) than as true senolytics in vivo.
Post-UNITY
Following the ASPIRE readout, UNITY stockholders voted to approve liquidation and dissolution in September 2025. The structural problems the company faced echo those of sirtuin: a mechanism with strong genetic mouse evidence did not translate into clinical separation from comparator on hard endpoints in human disease. The senolytic field did not collapse with the failure of UNITY, but has since split along two tracks that both avoid pitching directly against established standards of care.
The commercial track is exemplified by Rubedo Life Sciences, whose lead candidate RLS-1496 is a topical GPX4 modulator (inducing ferroptosis specifically in senescent cells rather than apoptosis); the compound met its safety endpoint in a European Phase 1 study and received FDA IND clearance in September 2025 for a US Phase 1b/2a trial in actinic keratosis, a localized, biopsy-accessible dermatologic indication that allows efficacy to be measured against a clear lesion-clearance endpoint rather than against an existing systemic therapy.
The academic track is led by James Kirkland, one of the field's founders, who runs investigator-initiated trials using off-patent senolytic combinations (most prominently dasatinib plus quercetin (D+Q)) across multiple disease indications, including diabetic kidney disease, idiopathic pulmonary fibrosis (Justice et al., 2019), osteoporosis, and the STOP-Sepsis Phase 2 trial using fisetin in older sepsis survivors.
Neither track is positioned to test the original senolytic hypothesis (that clearing senescent cells systemically extends healthspan in healthy older adults), and both implicitly concede that the path to clinical validation runs through narrow disease indications with conventional efficacy endpoints, not through aging as a construct.
In each of these cases, early testing in preclinical trials and testing on mice showed strong results, leading to optimistic funding rounds. In each case, clinical trials in humans failed to show the same results, leading both external and pharmaceutical industry funding to turn in other directions.
Aging is Not an FDA Indication
The vast majority of federally regulated drugs have specific biochemical targets, or pathways across one or multiple human organ systems (including the endocrine system, immune system, and nervous system, among others). These drugs also have specific disease or condition targets, or “indications,” defined as the specific, officially recognized medical purpose for which a drug, biological product, or medical device can be prescribed and marketed. In the official indications and usage guidance document from the FDA, the agency specifies that any approved drug’s published indications details should be scoped to “the disease or condition, or manifestation or symptoms thereof, for which the drug is approved, as well as whether the drug is indicated for the treatment, prevention, mitigation, cure, or diagnosis of that disease or condition, including relief of symptoms.”
Critically, the FDA does not recognize aging among the diseases and conditions for which treatments may be trialed and approved, though it does acknowledge myriad conditions associated with advanced age. This means that researchers studying treatments for aging need to select a specific indication for their therapies to target as a proxy for aging in general. Such indications can be challenging to select because clinical trials last months to years at most, while many aging-related mechanisms operate over entire lifetimes.
There are three primary layers of indications that are used in the field of anti-aging therapeutics for clinical trials: composite-endpoint trials, biomarkers and epigenetic clocks, and proxy disease indications.
Composite-Endpoint Trials
Composite-endpoint trials are clinical studies that combine multiple individual outcomes into a single primary endpoint, where a participant is counted as having an "event" if any one of the component outcomes occurs. Researchers favor this approach largely for statistical and practical reasons: rare outcomes like death require enormous sample sizes and long follow-up to detect treatment differences, so combining several related outcomes raises event rates and allows trials to reach adequate statistical power with fewer participants, less time, and less expense. Composites can also capture the overall burden of a disease more holistically when a treatment plausibly affects multiple outcomes through a shared mechanism.
Composite-endpoint trials can be controversial when poorly constructed because the overall result of the trial is often driven by the most frequent but least important endpoint while the most important endpoint shows no effect. Combining outcomes of very different severity risks treating more severe outcomes as equivalent to those that are less impactful to lifespan or healthspan. A treatment might also reduce one endpoint while increasing another, with the composite masking this divergence.
Reporting guidelines recommend that endpoints be of similar importance to patients, occur with similar frequency, and respond similarly to the intervention, and that each component always be reported separately alongside the composite so reviewers can determine whether the headline result reflects a real effect on what matters most. Some newer trials address these criticisms with hierarchical composites, such as the win ratio method, which rank outcomes by severity rather than treating them as equivalent.
TAME
One of the most widely discussed clinical trials of aging is the TAME (Targeting Aging with Metformin) trial, a proposed large-scale, multi-center, randomized placebo-controlled study designed in 2015 by Nir Barzilai at the Albert Einstein College of Medicine. The study would test whether the onset of age-related diseases in a population of 3K non-diabetic older adults over six years could be delayed by metformin, a cheap, widely used diabetes drug.
The significance of the study is rooted in its regulatory ambition, not in the specific medication used; TAME was conceived as a proof-of-concept trial to convince the FDA to recognize aging itself as an indication, using a composite endpoint of major age-related outcomes (cardiovascular disease, cancer, dementia, and death) to demonstrate that a single intervention can delay multiple diseases simultaneously. The composite endpoint components were chosen specifically because no individual age-related disease would accrue enough events to be statistically tractable in that timeframe
The FDA approved the design of the trial in 2015, but progress on starting the research was stalled by a lack of commercial funding because aging is not recognized as an FDA indication (at one point, prior to the collapse of WeWork, Adam Neumann offered to pay for the entire trial).
ASPREE
Another consequential aging-related composite endpoints trial is ASPREE (Aspirin in Reducing Events in the Elderly), a large-scale, multi-center, randomized, double-blind placebo-controlled study led by John McNeil at Monash University in collaboration with the US National Institute on Aging. The study tested whether daily low-dose (100 mg) enteric-coated aspirin could extend healthy lifespan in a population of 19K community-dwelling older adults across 34 US and 16 Australian sites. This group, comprised of individuals free of cardiovascular disease, dementia, and physical disability at enrollment, with ages over 70 in Australia and the US, or over for US racial and ethnic minorities, was followed for a median of 4.7 years between 2010 and 2017.
ASPREE was conceived as the first major trial to use a composite outcome explicitly engineered to capture healthy lifespan in older adults, using "disability-free survival, " defined as time to first occurrence of death, incident dementia, or persistent physical disability, as a composite endpoint alternative to cardiovascular events alone. The composite was chosen specifically because aspirin's known benefits for cardiovascular events and risks as a blood thinner operate on different organ systems with different time courses, and no single-disease endpoint would capture the integrated effect on independent living.
Results published in NEJM in 2018 showed aspirin did not prolong disability-free survival versus placebo, and a numerically higher rate of all-cause mortality was observed in the aspirin arm, driven partly by cancer deaths, findings that reshaped USPSTF primary-prevention guidance for adults over 70 and that established disability-free survival as a viable composite for future geroscience trials. ASPREE is the closest existing methodological precedent for TAME and is the design most often cited when arguing that multi-outcome composites can be operationalized at scale in healthy older adults.
Look AHEAD
Another widely-cited template for studying lifestyle interventions against composite aging-related outcomes is the Look AHEAD (Action for Health in Diabetes) study, a multi-center, randomized controlled trial sponsored by the NIH and conducted across 16 US sites starting in 2001. The study tested whether an intensive lifestyle intervention (caloric restriction, increased physical activity, behavioral counseling, targeting 7% weight loss) could reduce cardiovascular morbidity and mortality compared to a diabetes support and education control arm in a population of 5K adults aged 45 to 76 with type 2 diabetes and overweight/obesity over a period of 13.5 years.
The original significance of the study was its composite cardiovascular primary endpoint (first occurrence of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for angina), which was at the time the standard composite design for cardiometabolic outcomes trials. The trial was stopped for futility in 2012 because the intervention failed to reduce the primary CV composite, despite producing durable weight loss and improvements in diabetes control, sleep apnea, depression, and quality of life.
Look AHEAD's significance today, however, has been as a proof of concept for geroscience-specific composite endpoints. Through the Look AHEAD Aging substudy and a series of secondary analyses, the original cohort has been re-evaluated against multimorbidity indices (typically nine chronic conditions including coronary disease, cancer, depression, and kidney disease) and deficit-accumulation frailty indices (38 functional, behavioral, and clinical features). These reanalyses showed that the intensive lifestyle arm had 6% lower frailty index scores and accrued 0.14 fewer age-related chronic diseases two decades after the trial, benefits invisible under the original CV-only endpoint.
LOY-002
The closest analog to a composite-endpoint-tested aging therapeutic receiving FDA approval is the acceptance of LOY-002, a life extension drug for dogs. Loyal, the maker of the medication, received the FDA’s “reasonable expectation of effectiveness” for LOY-002 in February 2025. Reasonable expectation of effectiveness is a conditional approval granted by the FDA to veterinary medicines that allows pharmaceutical companies to begin manufacturing and distributing products before full approval is granted. LOY-002’s approval was the first formal FDA signal that any drug could be approved with a lifespan-extension claim in any species.
LOY-002 was tested via the STAY study, a 4-year, double-blind, placebo-controlled trial enrolling over 1K senior dogs (over 10 years old) across 70 veterinary clinics, structured around two parallel endpoints: lifespan and a quality-of-life / frailty measurement built from the Canine Frailty Index (CFI) and Health-Related Quality of Life (HRQL) instruments. These endpoints were sufficient for conditional approval because the FDA Center for Veterinary Medicine's Expanded Conditional Approval (XCA) pathway does not require the same surrogate-endpoint qualification machinery that has stalled equivalent human trials.
Biomarkers & Epigenetic Clocks
Geroscientists are increasingly advocating for the FDA to accept biological age biomarkers as surrogate endpoints that would allow trials to test interventions against "aging" directly, rather than against the multi-year, multi-disease composites required by trials like TAME and ASPREE. Surrogate biomarker endpoints would dramatically reduce the size, cost, and duration of geroscience trials, making it feasible to run dose-finding studies, screen candidate gerotherapeutics in months rather than decades, and circumvent the regulatory deadlock created by the FDA's non-recognition of aging as an indication. Such biomarkers proposed as proxies for aging include DNA-methylation-based epigenetic clocks like Horvath, GrimAge, PhenoAge, and DunedinPACE, as well as plasma protein abundances, transcriptomic clocks, inflammatory or "inflammaging" markers, and telomere length, among others.
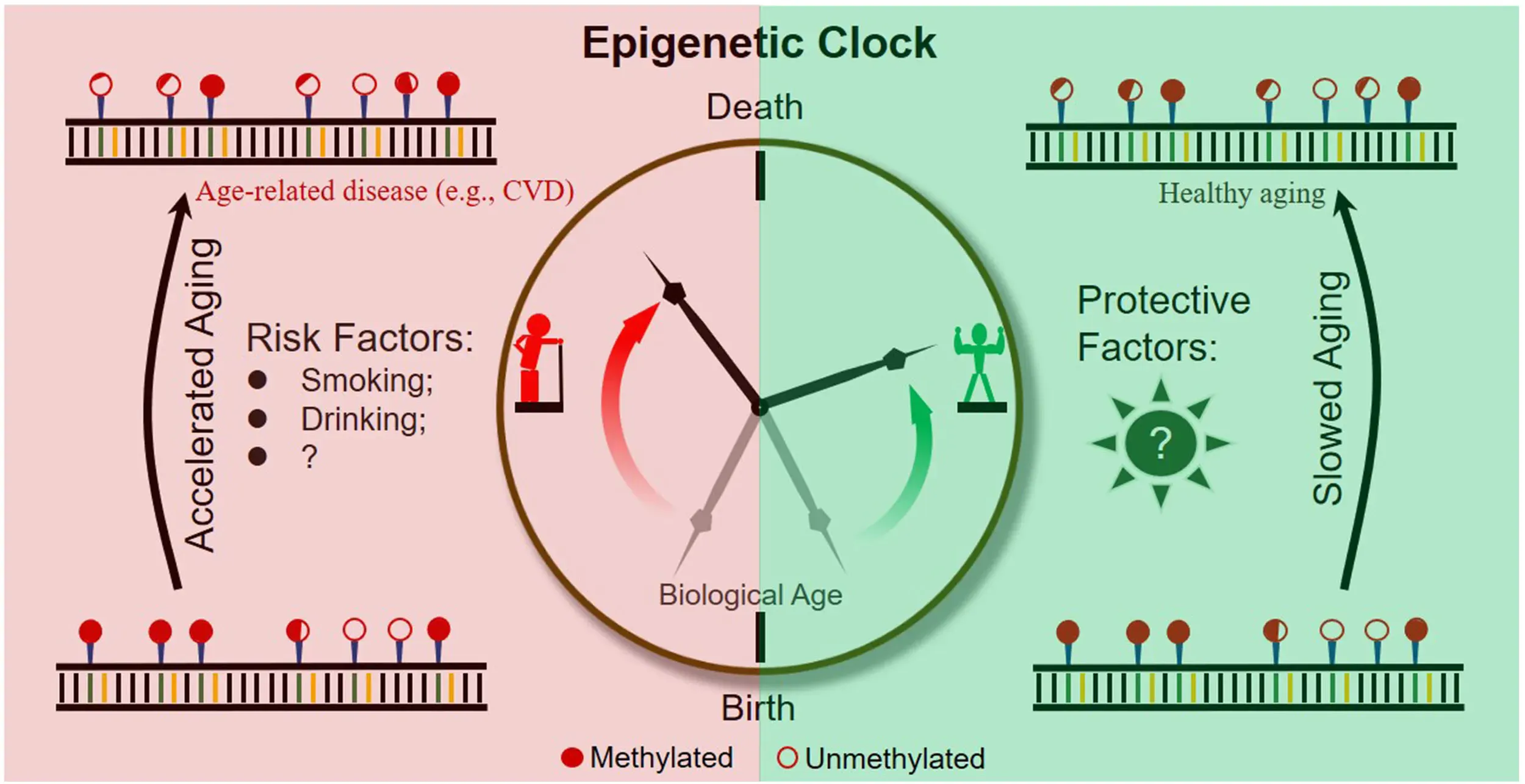
Source: Frontiers
None of these clocks is accepted as a surrogate endpoint by the FDA as of June 2026. In regulatory terms, they remain exploratory biomarkers used for hypothesis generation and secondary analyses, not for primary efficacy claims. The regulatory bar these biomarkers would need to clear to act as endpoints is high; the FDA's Biomarker Qualification Program has fully qualified five surrogate endpoints in its history. All five were cleared for specific diseases (drug-induced kidney injury, cardiovascular risk in particular contexts, and a handful of others), not for aging, which is not recognized as a disease. This means there is no single clinical outcome against which an aging biomarker could be validated as a surrogate without first defining one.
In addition to the regulatory challenge of biomarkers as endpoints, there remain scientific questions around their validity. Existing biomarkers may not actually correlate with causal aging biology. Ying et al. introduced the DamAge and AdaptAge clocks, which showed that conventional epigenetic clocks aggregate methylation sites driven by damaging changes and adaptive responses, meaning that an intervention can shift a clock without slowing the underlying aging process. This implies that a positive biomarker readout is not, on its own, evidence of a genuine geroprotective effect.
A 2024 consensus paper authored by multiple members of the geroscience field articulated the validation gap explicitly, demonstrating that existing clocks lack causal grounding, responsiveness to known geroprotective interventions in humans, and the mechanistic linkages to clinical outcomes required for surrogate qualification.
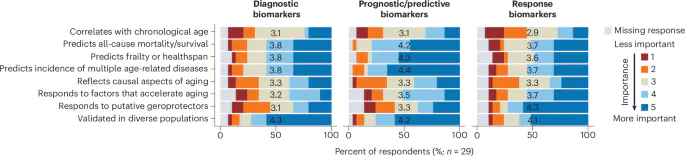
Source: Nature
Biomarkers are, as of June 2026, the preferred benchmark for evaluating aging interventions among longevity influencers and entrepreneurs like Brian Johnson. Programs like Johnson’s Project Blueprint aim to optimize a dashboard of biomarkers, treating changes in those biomarkers as evidence of slowing or reversing aging. Some of the biomarkers are reasonable proxies for healthspan, but others have been only weakly validated as individual-level intervention-response readouts.
Proxy Disease Indications
In some aging-related therapeutics trials, researchers select an age-related disease in order to run a standard trial of their treatment as a proxy for aging in general. This structure allows organizations to obtain approval for treatment of that specific disease, and potentially an expanded set of diseases in the future, but not for aging explicitly. Such proxy diseases have included diabetic macular edema (UNITY), Barth syndrome (Stealth), IPF (fisetin), Alzheimer’s (YouthBio, EVOKE), frailty, NAION + glaucoma (ER-100), and tuberous sclerosis epilepsy (Aeovian). As of June 2026, this is the only viable regulatory path to FDA approval, as component-endpoint trials and biomarkets do not identify indications that the FDA recognizes.
Apoptosis Inhibitor of Macrophage (AIM)
Similar to the LOY-002 therapy developed for dogs is the AIM (Apoptosis Inhibitor of Macrophage) program, which has produced what may become the first protein-replacement therapy targeting a species-specific aging mechanism in a companion animal. AIM (also called CD5L) is a circulating macrophage-derived protein that normally clears cellular debris and damaged cell material from organs. Researchers have shown that cats carry a genetic variant in which AIM binds too tightly to IgM and fails to detach when needed, which means the feline kidney cannot clear tubular debris effectively and accumulates damage. This appears to be the mechanistic explanation for why chronic kidney disease affects 30% of cats by age 10 and is the leading cause of death in domestic cats.
The platform used for the therapy is a recombinant AIM (rAIM) intravenous therapy. The rAIM trial used disease-specific endpoints (CKD progression and CKD-related mortality), validated against established kidney biomarkers. The results of the trial, published in February 2026, reported that IV administration of rAIM significantly extended survival in cats with advanced CKD and halted progression to end-stage disease and the worsening of kidney biomarkers. This trial was not pitched as an "aging" trial but rather as a disease-indication trial for feline CKD, but because feline CKD is the rate-limiting cause of cat mortality, a successful disease-indication approval would function as a feline lifespan-extension therapy.
While Loyal had to invent a healthspan/quality-of-life endpoint structure (the Canine Frailty Index and HRQL) because no single disease accounts for enough canine mortality to be a tractable approval target, the rAIM program could use a conventional disease endpoint because one disease accounts for a disproportionate share of feline mortality.
The Science of Partial Reprogramming
Yamanaka factors
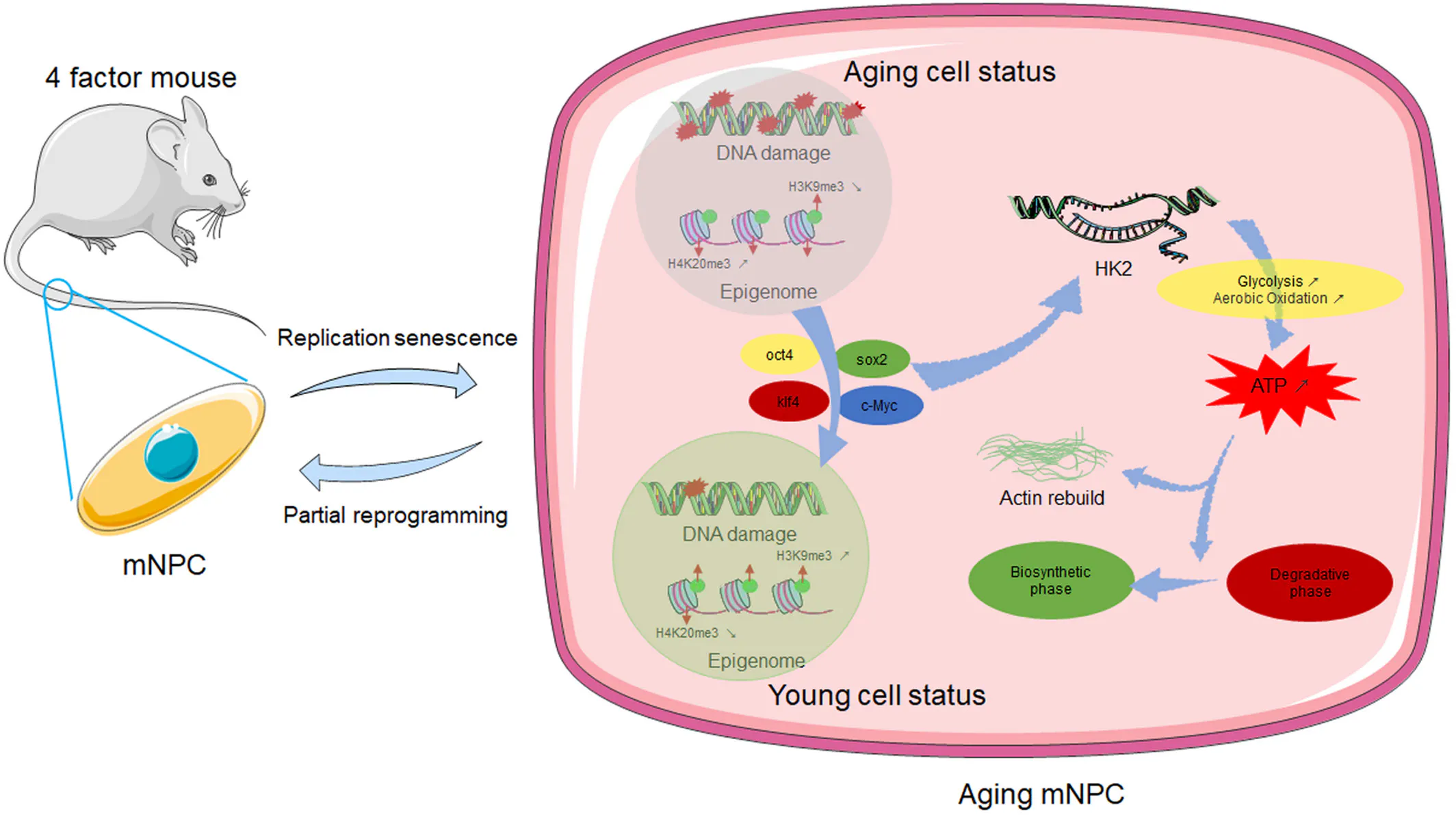
The most scientifically ambitious branch of geroscience targets a different layer of aging biology than senolytics, mTOR inhibition, or sirtuin activation: the epigenome itself. The platform descends from Yamanaka's Nobel-prize-winning discovery in 2006 that four transcription factors (OCT4, SOX2, KLF4, and c-MYC, or OSKM, the "Yamanaka factors") can revert adult somatic cells to a pluripotent embryonic-like state (iPSCs). Full reprogramming erases cellular identity and is tumorigenic in vivo, so the therapeutic field has focused on partial reprogramming: transient, controlled expression of a subset of factors (typically OSK, dropping the oncogenic c-MYC) that resets epigenetic age while stopping short of de-differentiation, leaving cellular identity and tissue-specific function intact.
Source: Aging Cell
Three foundational papers anchor the field:
Ocampo et al. (2016) showed that cyclic, short-pulse induction of OSKM extended lifespan in progeroid mice and ameliorated age-related hallmarks in wild-type mice without producing teratomas, establishing that the dose and duration of reprogramming can be tuned to a rejuvenation window short of pluripotency.
Lu et al. (2020) showed that AAV-delivered OSK restored youthful DNA methylation patterns in mouse retinal ganglion cells, promoted axon regeneration after optic nerve crush injury, and reversed vision loss in a glaucoma model and in aged mice.
Yang et al. (2023) introduced the "ICE" (Inducible Changes to the Epigenome) mouse model and the Information Theory of Aging, which frames aging as a reversible loss of epigenetic information rather than purely as the accumulation of molecular damage. It is important to flag that the Information Theory is one framework among several competing accounts of aging biology, not field consensus, but it is the theoretical scaffold most directly motivating partial-reprogramming therapeutics.
The central technical risk with partial reprogramming is tumorigenicity. Continuous expression of the four Yamanaka factors (OSKM) drives cells past partial reprogramming and into full pluripotency, producing teratomas in vivo within weeks. This finding was first established in Abad et al., Nature 2013, which showed that inducible whole-body OSKM expression in adult mice produced teratomas in multiple organs and was lethal when sustained.
This is why every reprogramming program currently in or near the clinic depends on tight temporal control: short, controlled pulses of factor expression that achieve epigenetic rejuvenation without crossing the threshold into pluripotency. The Phase 1 trials launching now are, in significant part, tests of whether these temporal-control mechanisms work as predicted in humans.
The mechanisms proposed vary but share the same underlying logic: dose and duration must be tunable, and the window of factor expression must close before cells lose identity (doxycycline-inducible AAV promoters (ER-100), mRNA pulses delivered by lipid nanoparticles that degrade within days (NewLimit), tissue-restricted promoters that limit expression to specific cell populations (YouthBio's neuron-specific YB002), and c-MYC omission (the OSK protocol used by Sinclair and Life Biosciences, which drops the most oncogenic factor entirely)).
ER-100
ER-100 received FDA clearance on January 15, 2026 (announced January 28, trial registered as NCT07290244). It is the first Yamanaka-factor partial-reprogramming therapy ever authorized for human testing.
The Phase 1 trial design enrolls up to 18 patients aged 40–85 (12 with open-angle glaucoma and 6 with NAION) and delivers an intravitreal AAV gene therapy carrying OCT4/SOX2/KLF4 under a doxycycline-controlled promoter, giving an 8-week activation window controlled by oral doxycycline dosing. The c-MYC factor is deliberately omitted to reduce tumor risk. The two indications, glaucoma and NAION ("stroke of the eye"), were chosen because both involve irreversible retinal ganglion cell death and have no disease-modifying therapy. The protocol includes five-year safety follow-up.
Future Paths for Reprogramming
While ER-100 is the first human anti-aging therapeutic to gain FDA approval for clinical trials in humans, it is only one of several programs making progress towards human testing and dosing.
Altos Labs
Altos Labs launched in January 2022 with over $3 billion in initial funding, the single largest biotech startup launch in history. The company’s team and research were built around founding scientist Juan Carlos Izpisua Belmonte (co-author of the 2016 Cell paper on cyclic OSKM extended lifespan), with Shinya Yamanaka as senior scientific advisor and a board roster of recruited academic leaders including Wolf Reik, Peter Walter, and Rick Klausner, as well as Nobel laureates Frances Arnold, Jennifer Doudna, and David Baltimore. In August 2025, Altos appointed Joan Mannick as Chief Medical Officer (the same Mannick who ran the Novartis/resTORbio mTOR trials in elderly immunity), the strongest signal that the company is preparing for clinical translation.
In October 2025, Belmonte publicly pivoted the company's near-term clinical focus toward ex vivo reprogramming of discarded donor organs, using normothermic perfusion machines to keep harvested livers, kidneys, and other organs alive outside the body while reprogramming factors are applied to restore function. The strategy sidesteps the principal regulatory and safety obstacles to in vivo reprogramming (tumorigenicity, systemic delivery, lack of validated aging endpoints) by treating organ rejuvenation as a transplant-supply problem rather than an aging-as-indication problem.
NewLimit
NewLimit was co-founded in 2021 by Coinbase CEO Brian Armstrong, former GV partner Blake Byers, and Stanford stem cell biologist Jacob Kimmel. NewLimit's strategy is technically distinct from Life Biosciences' and Altos's: rather than AAV-delivered Yamanaka factors, the lead asset uses lipid nanoparticles to deliver mRNA encoding novel transcription factor combinations. These combinations are identified through an AI-driven high-throughput screen called the Discovery Engine that has tested thousands of factor combinations on aged human hepatocytes and T cells. The lead program targets the aging liver, based on findings showing that prototype medicines have restored the ability of aged hepatocytes to process fat and alcohol in vitro. As of November 2025, the company planned its first-in-human trials to begin within the next few years.
YouthBio Therapeutics
YouthBio Therapeutics, founded in 2020 by Yuri Deigin, with David Sinclair as a co-founder and João Pedro de Magalhães as CSO, is focused on tissue-specific reprogramming in the brain. Its lead candidate, YB002, is a gene therapy delivering all four OSKM factors (including c-MYC) but restricted to neurons via neuron-specific promoters and AAV serotypes targeting the dentate gyrus, the hippocampal region central to learning and memory.
The preclinical rationale comes from a 2024 Ocampo collaboration showing that neuron-specific partial reprogramming in the dentate gyrus region of the brain improved learning and memory in aged mice and reduced amyloid-beta pathology in Alzheimer's models. In September 2025, YouthBio reported that the FDA agreed that existing preclinical data support the bioactivity of YB002 for first-in-human studies in Alzheimer's disease, with IND-enabling studies underway and a target of clinical trials within three years.
Retro Biosciences
Retro Biosciences, founded in 2021 by Joe Betts-LaCroix, has set the field's most explicit healthspan target: extending healthy human lifespan by 10 years. The company is pursuing multiple parallel platforms, inclduing partial cellular reprogramming and enhanced autophagy.
The reprogramming program is distinctive for its deep AI integration: in collaboration with OpenAI, Retro helped develop GPT-4b micro, a custom protein-design model that reportedly produced novel Yamanaka-factor variants 50 times more effective at inducing reprogramming markers than the wild-type proteins, according to results published with OpenAI in early 2025. Retro's reprogramming program remains preclinical as of early 2026, with no IND filing or human trial yet announced. The company’s two partial reprogramming therapeutics in pipeline (RTR888 for CNS conditions, intended to replenish the brain's resident immune cells in neurodegenerative disease; RTR890 for blood disorders, including leukemia) rest on the same iPSC platform from Yamanaka's original work but use full reprogramming ex vivo (producing genuine pluripotent cells, then differentiating them into specific cell types for transplant) rather than partial reprogramming in vivo.
Retro began its first trial in Australia in late 2025, an Alzheimer's program aimed at clearing protein aggregates from the brain, closer to an autophagy intervention than to direct reprogramming. The trials is testing RTR242, a small molecule designed to enhance the cellular waste-clearance pathway implicated as one of the canonical hallmarks of aging. Autophagy enhancement is mechanistically adjacent to (but distinct from) reprogramming: it targets the lysosomal degradation of damaged proteins and organelles rather than the epigenome, and it sits closer to the rapamycin/mTOR mechanism than to the OSK/Yamanaka mechanism.
The company raised a $180 million investment from Sam Altman in 2022, at the time the largest individual investment in a longevity company, as part of its seed funding. As of June 2026, the company is reportedly raising a Series A at a $1.8 billion valuation, with Altman participating.
Outlook
Beyond partial reprogramming, several adjacent technologies are being explored as possible tenets of anti-aging therapeutics.
Accidental Geroprotectors
The most consequential development in the anti-aging space in recent years was not produced by the longevity field at all, but in treatments of diseases that, either directly or via comorbidities, contribute to significant percentages of deaths in older adults. GLP-1 receptor agonists like semaglutide and tirzepatide were developed for diabetes and obesity, but have begun generating the kind of cross-disease, population-scale benefit profile that geroscience trials like TAME were designed to demonstrate.
The SELECT trial reported a 20% reduction in major adverse cardiovascular events in non-diabetic obese patients, and a July 2025 medRxiv preprint reported that semaglutide reduced PCGrimAge biological age by 3.1 years in HIV lipohypertrophy patients, the first randomized clinical evidence that a widely used drug moves an epigenetic clock. While this class of drugs decreases multiple aging-relevant biomarkers, its members may still produce a complicated net healthspan picture in older adults, with the medications causing significant muscle and bone loss that may accelerate aspects of frailty in older adults, and Phase 3 trials for reduction in Alzheimer's progression showing insignificant results.
Similar developments in treatments for coronary heart disease, which accounts for 24% of all deaths in the US for individuals above 25, have strengthened the case that indication-specific medicines are geroprotectors. In May 2026, Eli Lilly reported Phase 1b interim results for VERVE-102, an in vivo CRISPR base editor that permanently inactivates a gene associated with LDL cholesterol. A single dose produced dose-dependent PCSK9 reductions of 51–88% and LDL-C reductions up to 62%, sustained over 18 months of follow-up, with no treatment-related serious adverse events. The anti-aging mechanism is understood as the fact that humans who inherit loss-of-function PCSK9 variants have markedly lower lifetime LDL-C and an 88% reduction in coronary heart disease risk. VERVE-102, in effect, installs that protective variant pharmacologically as a single procedure.
Together, the GLP-1 cardiovascular data and the PCSK9 base-editing data describe a path to large-scale healthspan benefits that runs directly through conventional disease indications (obesity, dyslipidemia, atherosclerotic cardiovascular disease) rather than through aging as a regulatory or biological construct.
NAD+ Precursors
Nicotinamide mononucleotide (NMN) and nicotinamide riboside (NR) are the most heavily marketed but least clinically validated category in the anti-aging space. A Zhang 2024 meta-analysis of 12 NMN trials in Critical Reviews in Food Science and Nutrition found that blood NAD+ levels rose with supplementation but lipid, glucose, and BMI measurements did not move. Charles Brenner, who discovered NR in 2004, has become the loudest skeptic of his own field, noting that after twenty years and dozens of clinical trials, raising blood NAD has not translated into clinically significant results. NMN nonetheless remains a multi-billion-dollar supplement category, and Sinclair and Imai continue publishing positive mouse data on NAD+ restoration extending healthspan.
Thymic Regeneration
The thymus is the primary lymphoid organ where T cell progenitors from the bone marrow mature, undergo positive and negative selection against self-antigens, and emerge as naive T cells capable of recognizing novel pathogens; it begins involuting at puberty and is largely replaced by adipose tissue by middle age, with naive T cell output dropping by roughly 90% by age 70. The resulting immunosenescence is a central driver of the age-related rise in infection mortality, cancer incidence, vaccine non-response, and autoimmune disregulation. The mechanistic premise of thymic regeneration therapeutics is that the thymic epithelial compartment retains the capacity to be reactivated by the right signaling inputs (most prominently growth hormone, which acts via IGF-1 on thymic epithelial cells to restore stromal architecture and re-open the niche for thymocyte development) and that re-establishing naive T cell output even partially in older adults would push the immune compartment back toward a younger functional phenotype.
Intervene Immune's TRIIM-X trial (NCT04375657), based at the Lundquist Institute, is attempting to replicate the most-cited single human result in the modern longevity field: Greg Fahy 2019 (Aging Cell), which reported that a combination of growth hormone, metformin, and DHEA reversed 2.5 years of epigenetic age (measured via the Horvath clock) and produced apparent thymic regeneration on MRI in healthy older men. TRIIM-X has enrolled approximately 24 of a planned 80 participants. The original TRIIM study was open-label, with no placebo control, leading to demand for a replication study; the broader thymic involution literature has long established that thymic atrophy is a central driver of age-related immune decline, but until TRIIM-X is completed these claims are yet to be validated.
Mitochondrial Therapeutics
Mitochondrial dysfunction is one of the canonical hallmarks of aging (López-Otín et al., Cell 2023), and the field reached a regulatory milestone in September 2025 when Stealth BioTherapeutics' elamipretide (FORZINITY) became the first FDA-approved mitochondria-targeted therapeutic, indicated for Barth syndrome. Elamipretide is a cardiolipin-binding peptide that stabilizes the inner mitochondrial membrane and improves electron transport chain efficiency; the approval validates the mechanism in a disease where the mitochondrial defect is causal. However, Barth is an ultra-rare pediatric genetic disease, and the approval validates a mechanism, not aging-as-indication. Stealth's earlier ReCLAIM-2 Phase 2 trial in age-related macular degeneration (a much more common age-driven condition) produced ambiguous data despite strong mechanistic rationale, leaving the outlook for the therapy unclear.
The Funding Paradox
Longevity biotech raised approximately $3.7 billion across 49 deals in Q1 2026, 56% above Q1 2025 and the largest quarter on record. In 2025, AbbVie ended its 11-year, $1.75 billion partnership with Calico (Google/Alphabet's flagship aging bet), UNITY dissolved, and the GLP-1 Alzheimer's trial missed. The field is simultaneously breaking funding records and absorbing its biggest public failures, with capital flowing into platform bets concurrently with the write-down of the previous generation of platform bets. Whether that pattern reflects rational re-allocation toward better science or a recurring cycle of hype and disappointment is one open question ER-100's Phase 1 readout will begin to answer.
As of June 2026, the state of anti-aging research and therapeutics remains in flux, with the hurdle of clearing FDA standards for clinical trials remaining the primary challenge for the field. Unless FDA standards change to accommodate such trials specifically, the path to funding, clinical trials, and regulatory approval will remain uphill for anti-aging and longevity therapeutics developers. Despite this roadblock, the outlook for specific modalities, including partial reprogramming and GLP-1s, is as strong as any past anti-aging platform proposed. The outcomes of ongoing clinical trials like ER-100 may be turning points for the anti-aging field as a whole.